Cranial Nerve III: Oculomotor Nerve
What’s unique about the Oculomotor Nerve?
The Oculomotor Nerve has motor and parasympathetic functions. It connects to 4 out of the 6 extraocular muscles to move the eye, plus an additional muscle to lift the eyelid. Parasympathetically, it constricts the pupil and focuses the lens within the eye.
What is the function of the nerve?
Motor: Controls movement of 4 out of 6 extraocular muscles and a muscle to lift the eyelid
Parasympathetic: Construction of the pupil (decrease amount of light) and lens accommodation (shape-shifting the lens to maintain focus on an object that is either close up or far away)
What are the signs of dysfunction?
Signs of oculomotor dysfunction include:
• Ptosis, a down and outward gaze
• Mydriasis (dilated pupil in the affected eye)
It can be present at birth, or it may also occur later in life due to:
• Inadequate blood flow: Causes lack of oxygen that nerves need to function properly.
• Compression: Pressure on the nerve or within the cavernous sinus can create compression.
How might this nerve be impacted?
Conditions that may cause oculomotor dysfunction include:
• Brain aneurysm; an aneurysm of the posterior communicating artery can apply pressure to the nerve close to its emergence from the brainstem
• Brain tumor
• TBI
• Multiple Sclerosis (MS)
• Diabetes and high blood pressure
• Infections, including HIV and Lyme disease
• Migraine
How can you work with this nerve?
•Notice the tentorium, the brainstem, the sphenoid bone, the cavernous sinus, and the eye field and offer space for decompression for each
• Visualize the pathway, from the brainstem, moving through the tentorium and the superior orbital fissure of the sphenoid, and attaching to the various muscles of the eye
• Notice the quality of potency moving through the nerve
• Hold space for any held patterns to shift
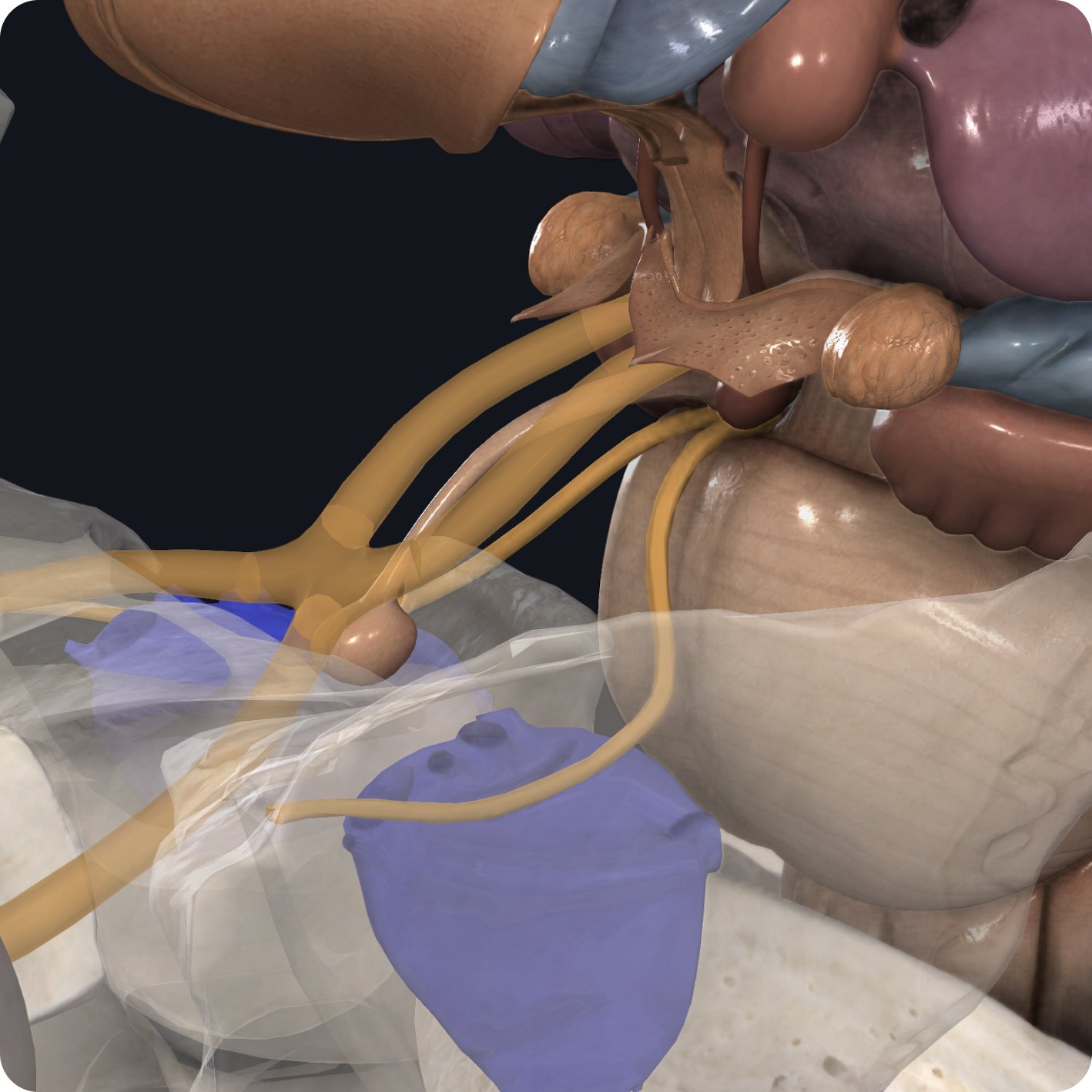
At the brainstem, a collection of both somatic and visceral motor axons exit on the anterior surface as the oculomotor nerve.

From here, the nerve runs anteriorly in the subarachnoid space, piercing the tentorium and passing through the wall of the cavernous sinus.

Upon exiting the cavernous sinus, the oculomotor nerve runs below the lesser wing of the sphenoid bone to enter the orbit through the superior orbital fissure.

As the nerve enters the orbit, it divides into its superior and inferior branches. Both branches will pass into the orbit within the boundaries of the common tendinous ring.

From here, the superior and inferior branches will pass anteriorly to supply the extraocular muscles of the eye.

The Levator Palpebrae Superioris muscle is responsible for elevating the eyelid.

The Superior Rectus muscle moves the eyeball superiorly or elevates it.

The Inferior Rectus muscle depresses and adducts the eyeball.

The Medial Rectus muscle abducts the eyeball, moving it towards the midline.

Finally, the Inferior Oblique muscle elevates, abducts and laterally rotates the eyeball.
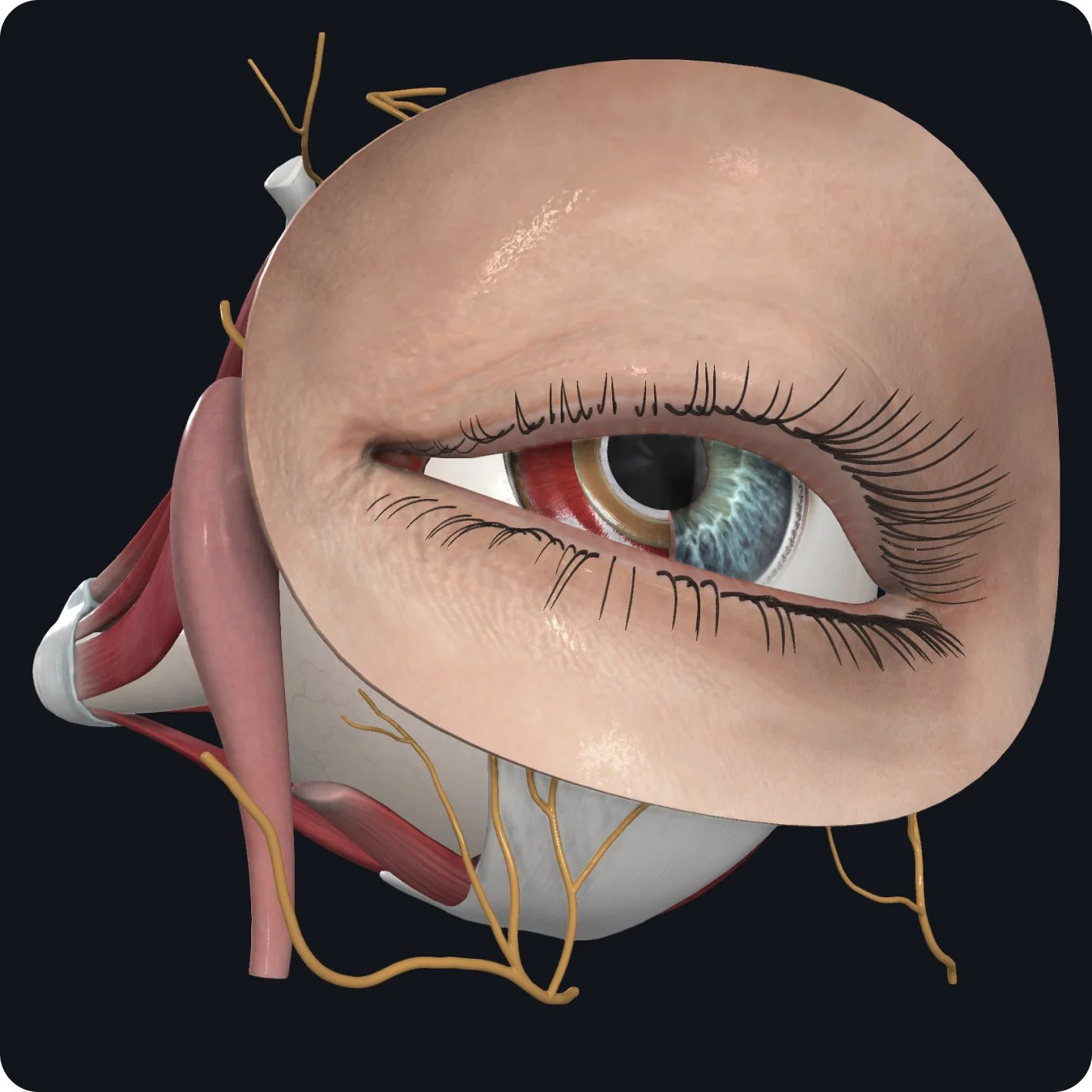
Innervation of the Sphincter Pupillae muscle allows for pupil constriction.

This nerve also innovates the ciliary muscles which when contracted alters the curvature of the lens and and allows an individual to focus.